When the arteries that supply blood to your heart become narrowed or blocked, the consequences can range from debilitating chest pain to a life-threatening heart attack. Angioplasty is a minimally invasive procedure that opens these blocked arteries and restores blood flow to the heart muscle — often within hours of a cardiac emergency, and without the need for open-heart surgery. At Vikram Heart Care Centre, angioplasty is performed by Dr Kushaal Vikram, a specialist cardiologist with extensive interventional experience.
Understanding Coronary Artery Disease
The heart is a muscle that works continuously, every minute of every day. Like all muscles, it requires a constant supply of oxygenated blood to function. This supply is delivered through three major coronary arteries and their branches that run across the surface of the heart.
Coronary artery disease (CAD) develops when fatty deposits — called plaques — build up inside the walls of these arteries over time. This process, known as atherosclerosis, gradually narrows the artery and reduces blood flow to the heart muscle. When a plaque ruptures, a blood clot can form rapidly at the site, causing a sudden and complete blockage — a heart attack.
Angioplasty directly addresses this problem by physically opening the narrowed or blocked artery from within.
What Is Angioplasty?
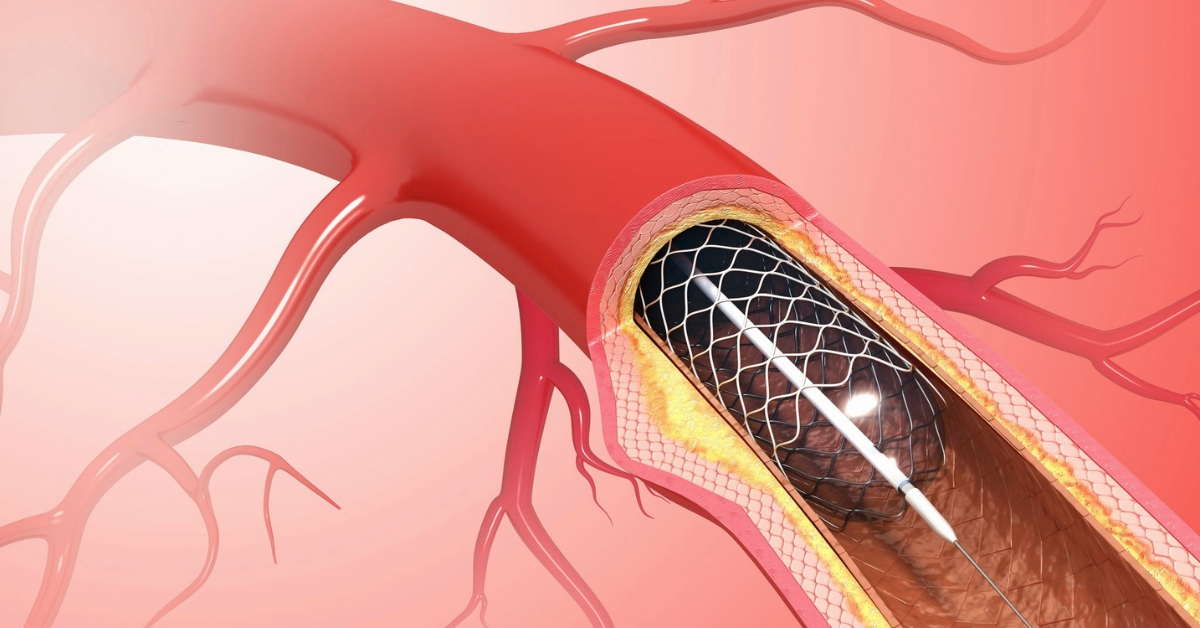
Angioplasty — formally known as Percutaneous Coronary Intervention (PCI) — is a catheter-based procedure performed in a specialised cardiac catheterisation laboratory (cath lab). It involves threading a thin, flexible tube (catheter) through a blood vessel in the wrist or groin up to the blocked coronary artery, then using a small balloon to compress the plaque against the artery wall and restore blood flow.
In the vast majority of cases, a stent — a small metal mesh tube — is also implanted at the site of the blockage to keep the artery open and prevent it from narrowing again.
Types of Angioplasty
Balloon Angioplasty The original technique. A tiny balloon at the tip of the catheter is inflated at the site of the blockage, compressing the plaque and widening the artery. Balloon angioplasty alone is now rarely performed without stent placement, as arteries tend to re-narrow (restenose) without additional support.
Bare Metal Stent (BMS) Implantation A metal mesh stent is deployed at the site of the blockage after balloon dilation to scaffold the artery open. Provides structural support but carries a moderate risk of restenosis due to tissue ingrowth into the stent.
Drug-Eluting Stent (DES) Implantation The current standard of care. A stent coated with a medication that is slowly released into the artery wall, inhibiting the growth of scar tissue and significantly reducing the risk of restenosis compared to bare metal stents. Most contemporary angioplasty procedures use drug-eluting stents.
Primary PCI (Emergency Angioplasty) Angioplasty performed on an emergency basis for a heart attack (STEMI — ST-Elevation Myocardial Infarction). Time is critical — every minute of delay allows more heart muscle to die. Primary PCI is the gold standard treatment for heart attack when it can be performed promptly, restoring blood flow faster and more effectively than clot-dissolving medications alone.
Elective PCI Angioplasty performed on a planned basis for stable coronary artery disease causing significant symptoms (stable angina) that have not responded adequately to medications.
When Is Angioplasty Recommended?
Emergency Situations
- Acute STEMI (heart attack with complete artery blockage) — primary PCI is the treatment of choice and should be performed as rapidly as possible
- High-risk NSTEMI (heart attack without complete ST elevation) — urgent angioplasty may be recommended depending on the clinical picture
Planned / Elective Situations
- Stable angina with significant coronary artery narrowing causing limiting symptoms despite optimal medical therapy
- Significant coronary artery disease identified on angiography with evidence of reduced blood flow to the heart muscle (ischaemia)
- Previous coronary artery bypass graft with a blocked graft causing symptoms
The decision to proceed with angioplasty versus continued medical management or bypass surgery depends on several factors including the number and location of blockages, the degree of ischaemia, heart function, and the patient’s overall health. Dr Kushaal Vikram will discuss all options and guide the most appropriate decision for your situation.
The Procedure: What to Expect
Before the Procedure
- Blood tests, ECG, and echocardiogram are performed to assess baseline cardiac function
- Medications including antiplatelet agents (aspirin and a second antiplatelet drug such as clopidogrel or ticagrelor) are started before the procedure
- You will be asked to fast for a period before the procedure if it is planned
- Contrast dye allergy and kidney function are assessed, as contrast is used during the procedure
During the Procedure
Angioplasty is performed in the cardiac catheterisation laboratory under local anaesthesia. You will be awake throughout but will feel minimal discomfort.
The procedure steps:
- A local anaesthetic is injected at the access site — typically the wrist (radial artery) or groin (femoral artery)
- A small introducer sheath is inserted into the artery
- A guide catheter is threaded through the sheath and navigated under X-ray guidance to the opening of the blocked coronary artery
- Contrast dye is injected to visualise the blockage (coronary angiography)
- A very fine guidewire is passed through the blockage
- A balloon catheter is advanced over the guidewire to the site of the narrowing and inflated to compress the plaque
- A stent is deployed at the same site to scaffold the artery open
- Final contrast injections confirm the blockage has been successfully treated and blood flow restored
The procedure typically takes 30 minutes to 2 hours depending on the complexity and number of vessels treated.
After the Procedure
- You will be monitored in a recovery area for several hours
- The access site in the wrist or groin will be compressed and bandaged
- Most patients who undergo elective angioplasty are discharged the same day or the following morning
- Patients treated for a heart attack will remain in hospital for monitoring for 2 to 5 days depending on their condition
Recovery and Life After Angioplasty
Recovery from angioplasty is significantly faster than open-heart surgery.
General recovery guidelines:
- Avoid heavy lifting or strenuous physical activity for at least 1 week after elective angioplasty
- The access site wound (wrist or groin) should be kept clean and dry
- Most patients can return to desk work within a few days
- Driving is usually restricted for 1 week after elective PCI and longer after a heart attack
- Sexual activity can typically be resumed within 1 to 2 weeks
Medications after angioplasty:
Dual antiplatelet therapy — aspirin combined with a second antiplatelet agent — is essential after stent implantation and must not be stopped without cardiology advice. Stopping these medications prematurely significantly increases the risk of stent thrombosis, a dangerous clot forming within the stent.
The duration of dual antiplatelet therapy depends on the type of stent, the indication for angioplasty, and other clinical factors — typically 6 to 12 months for drug-eluting stents, sometimes longer.
Other medications commonly prescribed after angioplasty include:
- Statins — to lower cholesterol and stabilise coronary plaques
- Beta-blockers — to reduce heart rate and workload
- ACE inhibitors or ARBs — to protect heart function
- Antihypertensives — to control blood pressure
Lifestyle modifications are equally important:
- Stop smoking completely and permanently
- Adopt a heart-healthy diet low in saturated fats, trans fats, and refined sugars
- Engage in regular moderate physical activity as advised by your cardiologist
- Achieve and maintain a healthy body weight
- Control blood pressure, diabetes, and cholesterol with medications and lifestyle
Angioplasty treats the blockage but does not cure the underlying coronary artery disease. Without lifestyle change and medical management, new blockages can develop in other arteries or in the same vessel.
Risks and Complications
Angioplasty is a well-established procedure with a strong safety record. However, as with any invasive procedure, risks exist and should be understood before consenting.
Common minor complications:
- Bruising or bleeding at the access site
- Allergic reaction to contrast dye (usually mild and manageable)
- Temporary kidney function impairment from contrast dye, particularly in patients with pre-existing kidney disease
Less common but serious complications:
- Stent thrombosis — a blood clot forming within the stent; risk is highest in the first days to weeks and is significantly reduced by antiplatelet therapy
- Re-narrowing of the artery (in-stent restenosis) — more common with bare metal stents than drug-eluting stents
- Heart attack during or after the procedure — rare but possible, particularly in complex cases
- Stroke — rare
- Artery dissection — a tear in the artery wall during the procedure, usually manageable with additional stenting
- Emergency bypass surgery — required in very rare cases where angioplasty cannot be completed safely
Your cardiologist will discuss the specific risks relevant to your case before the procedure.
Angioplasty vs Bypass Surgery
Both angioplasty and coronary artery bypass grafting (CABG) are established treatments for significant coronary artery disease. The choice between them depends on the nature and extent of the disease.
Angioplasty is generally preferred when:
- Single vessel or two-vessel disease is present
- The blockage is in a location technically suitable for stenting
- The patient prefers to avoid open-heart surgery
- Emergency treatment of a heart attack is required
Bypass surgery may be preferred when:
- Three-vessel disease or left main artery disease is present
- The anatomy is not suitable for stenting
- Diabetes is present alongside multi-vessel disease
- Previous angioplasty has not provided durable results
In many cases, a multidisciplinary discussion between the interventional cardiologist and cardiac surgeon determines the best approach. Dr Kushaal Vikram will guide you through this decision with clear, honest advice tailored to your specific anatomy and clinical situation.
Frequently Asked Questions
Q: Is angioplasty open-heart surgery?
No. Angioplasty is a minimally invasive catheter-based procedure. It does not involve opening the chest or stopping the heart. It is performed through a small puncture in the wrist or groin, under local anaesthesia, and most patients go home within 24 hours.
Q: Will I feel the balloon being inflated inside my artery?
You may feel a brief pressure sensation or slight chest tightness when the balloon is inflated, but this is typically brief and well tolerated. The procedure is performed under local anaesthesia at the access site, and sedation is available if needed.
Q: How long does a stent last?
A stent is a permanent implant — it stays in the artery for life. Drug-eluting stents have excellent long-term results, with restenosis rates of less than 5 to 10% at one year. The stent itself does not wear out, but the underlying coronary artery disease can continue to progress in other vessels if risk factors are not addressed.
Q: Can I have an MRI scan after a stent has been implanted?
Modern coronary stents are made from MRI-compatible materials and are generally safe for MRI scanning. It is advisable to wait at least 6 weeks after implantation before undergoing an MRI, and you should always inform the radiology team of your stent before any MRI procedure.
Q: What happens if the stent becomes blocked again?
Re-narrowing within a stent (in-stent restenosis) or stent thrombosis are manageable complications. Options include repeat angioplasty with a new drug-eluting stent or drug-coated balloon, or in some cases, referral for bypass surgery. Regular follow-up with your cardiologist and strict adherence to antiplatelet medications are the best ways to reduce this risk.
Q: My doctor has recommended both angioplasty and bypass surgery. How do I decide?
This is a decision that should be made jointly with your cardiologist and cardiac surgeon, based on a detailed review of your angiogram, your overall health, and your personal preferences. Both procedures have proven benefits in appropriate patient populations. Dr Kushaal Vikram will ensure you have all the information needed to make the right choice for your situation.
Q: Is angioplasty available in Patna?
Yes. Angioplasty and percutaneous coronary intervention are performed at Vikram Heart Care Centre, Dr K K Kantha Memorial Hospital, Patna, by Dr Kushaal Vikram.
Book a Consultation
If you have been diagnosed with coronary artery disease, are experiencing chest pain or breathlessness on exertion, or have been advised to consider angioplasty, a specialist consultation with Dr Kushaal Vikram is your next step.
📞 +91 893 583 4142 | +91 886 400 4584
📍 21 B/3, Patliputra Colony, Near Pataliputra Golambar, Opp. UNICEF Building, Patna 800 013
🌐 Book online at kanthahospital.com