If the ECG tells you about the heart’s electrical activity, the echocardiogram shows you the heart itself — its structure, its movement, its valves, and the way blood flows through its chambers in real time. Echocardiography is the single most important imaging tool in cardiology, providing a level of detail about the heart’s anatomy and function that no other bedside investigation can match. At Vikram Heart Care Centre, echocardiography is performed and interpreted by Dr Kushaal Vikram, bringing specialist-level cardiac imaging to patients in Patna.
What Is Echocardiography?
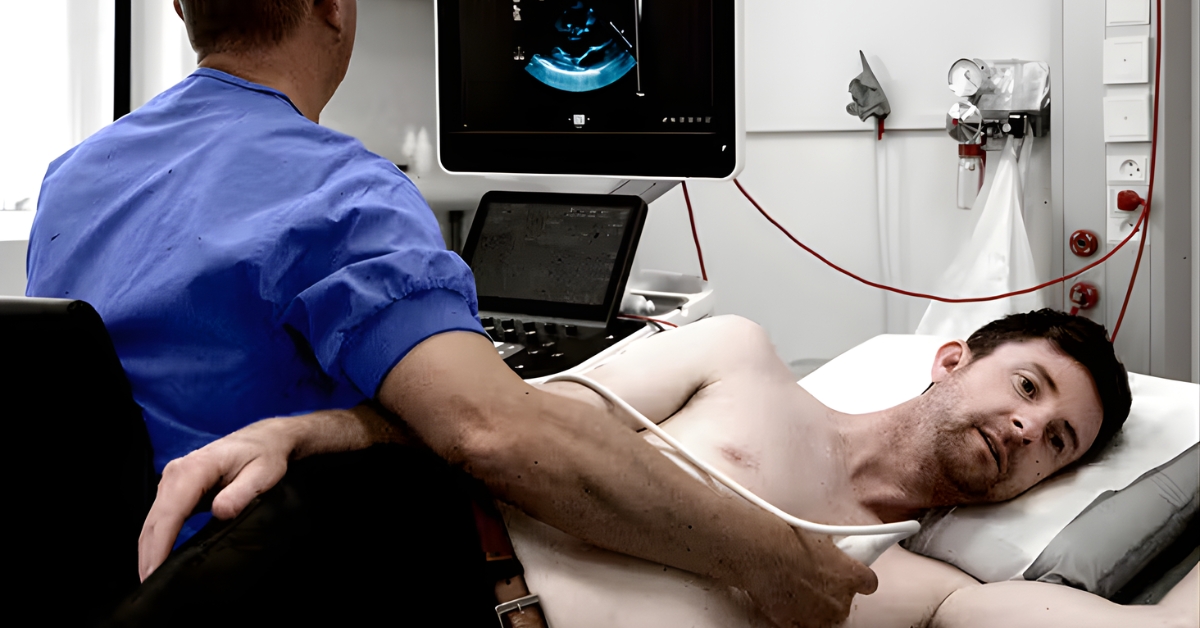
Echocardiography — commonly called an “echo” — is an ultrasound scan of the heart. It uses high-frequency sound waves to create real-time images of the heart’s structure and function. Just as obstetric ultrasound shows an unborn baby moving in the womb, echocardiography shows the beating heart — its chambers filling and emptying, its valves opening and closing, and blood moving through its cavities.
There is no radiation involved. The technology is safe, non-invasive, and can be performed at the bedside or in an outpatient setting. It provides information that would otherwise require invasive testing or expensive imaging such as MRI or CT.
What Does an Echocardiogram Assess?
A comprehensive echocardiogram evaluates virtually every aspect of cardiac anatomy and function.
Structure and Size
- Dimensions of all four heart chambers — left and right ventricles, left and right atria
- Wall thickness of the ventricles — thickening indicates hypertrophy from hypertension or other causes
- Overall cardiac size and any enlargement (cardiomegaly)
Ventricular Function
- Left Ventricular Ejection Fraction (LVEF) — the percentage of blood ejected from the left ventricle with each beat; the single most important measure of cardiac pump function; a normal EF is 55% or above
- Wall Motion Analysis — each segment of the left ventricle is assessed individually; reduced or absent movement in a segment indicates ischaemia or prior infarction
- Diastolic Function — how well the ventricle relaxes and fills between beats; diastolic dysfunction is a common finding in hypertension and ageing and is associated with heart failure with preserved ejection fraction (HFpEF)
- Right ventricular size and function — important in pulmonary hypertension, right heart failure, and congenital disease
Valves All four heart valves are examined in detail:
- Mitral Valve — opens to allow blood into the left ventricle; can develop stenosis (narrowing) or regurgitation (leaking)
- Aortic Valve — opens to allow blood out of the left ventricle into the aorta; aortic stenosis is the most common valvular disease in older adults
- Tricuspid Valve — between the right atrium and right ventricle; tricuspid regurgitation provides an estimate of pulmonary artery pressure
- Pulmonary Valve — least commonly diseased; important in congenital heart conditions
Pericardium
- Detection of pericardial effusion — fluid around the heart
- Assessment of cardiac tamponade — compression of the heart by accumulated fluid, a life-threatening emergency
- Signs of constrictive pericarditis
Aorta
- Dimension of the aortic root and ascending aorta
- Detection of aortic dilatation or aneurysm
- Signs of aortic dissection
Intracardiac Structures
- Detection of clots (thrombus) within the heart chambers — particularly in the left atrial appendage in atrial fibrillation
- Tumours within the heart (myxomas and other masses)
- Vegetations on valves in infective endocarditis
- Congenital defects — atrial septal defects (ASD), ventricular septal defects (VSD), patent foramen ovale (PFO), and more complex structural abnormalities
Types of Echocardiography
Transthoracic Echocardiogram (TTE) The standard echo performed from outside the chest. An ultrasound probe is placed on the chest wall at several positions and angled to obtain views of different parts of the heart. It is completely non-invasive and requires no special preparation. This is the routine first-line echo performed in most clinical situations.
Doppler Echocardiography An essential component of every standard echo. Doppler technology measures the speed and direction of blood flow through the heart’s chambers and valves. It quantifies the severity of valve stenosis and regurgitation, measures pressure gradients across narrowed valves, estimates pulmonary artery pressure, and assesses diastolic function.
Colour Doppler An extension of Doppler imaging that colour-codes blood flow — typically showing flow towards the probe in red and flow away in blue. It makes abnormal flow patterns such as valve regurgitation immediately visible and allows rapid identification of intracardiac shunts.
Tissue Doppler Imaging (TDI) Measures the velocity of the myocardium itself rather than blood flow, providing detailed assessment of ventricular relaxation and diastolic function.
Stress Echocardiography An echo performed both at rest and during or immediately after physical exercise (treadmill or bicycle) or pharmacological stress (dobutamine infusion). The purpose is to detect areas of the heart that contract normally at rest but show reduced function under stress — indicating underlying coronary artery disease. It combines the haemodynamic information of a stress test with the structural imaging of echo.
Transoesophageal Echocardiography (TOE/TEE) A specialised echo in which the ultrasound probe is passed down the oesophagus (food pipe) to obtain images from immediately behind the heart. It provides far superior image quality for structures that are difficult to see from the chest wall — particularly the left atrial appendage (for clot detection before cardioversion), the mitral valve (before repair surgery), prosthetic valves, and the aorta. Performed under sedation.
Contrast Echocardiography A small amount of contrast agent (microbubbles) is injected intravenously to improve the definition of the left ventricular border and enhance Doppler signals. Useful when image quality from the standard echo is suboptimal.
Three-Dimensional (3D) Echocardiography Provides volumetric imaging of the heart’s chambers and valves, allowing more accurate measurements and detailed surgical planning — particularly for valve repair or replacement.
Conditions Diagnosed and Monitored with Echocardiography
Heart Failure Echo is the definitive test for diagnosing heart failure, distinguishing between heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF), and monitoring response to treatment.
Coronary Artery Disease Wall motion abnormalities at rest indicate prior myocardial infarction. Stress echocardiography detects ischaemia — areas at risk from coronary narrowing.
Valvular Heart Disease Echo is the gold standard for diagnosing, grading the severity of, and monitoring the progression of all forms of valve disease — stenosis and regurgitation of any valve.
Hypertension Echo detects left ventricular hypertrophy (the heart’s response to sustained high blood pressure) and diastolic dysfunction. Both are important independent predictors of cardiovascular risk beyond blood pressure measurement alone.
Cardiomyopathies
- Dilated Cardiomyopathy — enlarged, poorly contracting heart
- Hypertrophic Cardiomyopathy (HCM) — abnormal thickening of the heart muscle, often inherited; a cause of sudden death in young athletes
- Restrictive Cardiomyopathy — stiff heart muscle impairing filling
- Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
Infective Endocarditis Detection of vegetations (infected deposits) on heart valves and assessment of valvular destruction.
Pericardial Disease Detection of pericardial effusion and assessment of cardiac tamponade — a life-threatening situation requiring urgent drainage.
Congenital Heart Disease Echo is the primary imaging tool for diagnosing and monitoring congenital defects — in children and in adults with previously undiagnosed or repaired congenital conditions.
Atrial Fibrillation Assesses left atrial size (a determinant of success of cardioversion and ablation), ventricular function, and valve disease contributing to AF. TOE is used to exclude left atrial appendage thrombus before cardioversion.
Pulmonary Hypertension Tricuspid regurgitation velocity on Doppler provides an estimate of right ventricular systolic pressure, allowing non-invasive screening for pulmonary hypertension.
Aortic Disease Measurement of aortic root and ascending aorta dimensions for surveillance of aortic aneurysm and screening in conditions such as Marfan syndrome.
The Procedure: What to Expect
A standard transthoracic echocardiogram is entirely painless and comfortable.
What happens during the test:
- You will be asked to undress from the waist up and lie on an examination couch, initially on your back and then turned slightly onto your left side
- Electrodes are attached to monitor your ECG simultaneously during the scan
- A small amount of gel is applied to your chest — this is water-based, not harmful, and wipes off easily
- The sonographer or cardiologist places the ultrasound probe at several positions on your chest, applying gentle pressure to obtain optimal images
- You may be asked to breathe in, breathe out, or hold your breath briefly at certain points
- The scan takes approximately 30 to 45 minutes
- There is no pain, no needles, and no radiation
Results are reviewed and interpreted by Dr Kushaal Vikram and discussed with you at the appointment or communicated through your referring physician.
Preparation for an Echocardiogram
A standard transthoracic echocardiogram requires no special preparation.
- You may eat and drink normally beforehand
- Continue all your regular medications as usual
- Wear comfortable clothing that allows easy access to the chest
- Inform the team if you have a pacemaker or implanted defibrillator — this is safe but relevant to the images obtained
For a stress echocardiogram, specific preparation instructions (including fasting and medication adjustments) will be provided when your appointment is booked.
Frequently Asked Questions
Q: Is echocardiography the same as a cardiac ultrasound?
Yes. Echocardiography is simply the medical term for an ultrasound scan specifically of the heart. The technology is the same ultrasound used in other parts of medicine, adapted and refined for cardiac imaging.
Q: Is the procedure painful or uncomfortable?
A standard transthoracic echo is completely painless. You may feel slight pressure from the probe, and the gel can feel cool on the skin. Some positions require you to turn on your side, which most patients find comfortable. There is no discomfort beyond these minor points.
Q: How long does an echo take?
A standard resting echo typically takes 30 to 45 minutes including set-up, scanning, and initial review. A stress echo or TOE takes longer and will be discussed with you when scheduled.
Q: My doctor said my echo showed a reduced ejection fraction. What does this mean?
Ejection fraction (EF) measures how well your left ventricle pumps blood out with each beat. A normal EF is 55% or above. A reduced EF indicates the heart is not pumping as effectively as it should — a condition called heart failure with reduced ejection fraction (HFrEF). This is a significant finding that requires specialist cardiology management, medication optimisation, and regular monitoring. It does not necessarily mean your condition cannot be improved — many patients respond well to appropriate treatment.
Q: Can an echo detect a blocked artery?
A standard resting echo cannot directly visualise the coronary arteries. However, it can detect the consequences of coronary artery disease — namely, areas of the heart wall that are not contracting normally due to previous heart attack or ongoing ischaemia. A stress echocardiogram is more sensitive for detecting ischaemia from coronary narrowing.
Q: I have been diagnosed with a heart murmur. Do I need an echo?
Yes. An echocardiogram is the standard investigation for evaluating a heart murmur. It identifies whether the murmur is caused by a structural valve abnormality, quantifies its severity, and determines whether any action is required. Many murmurs are innocent — but this can only be confirmed with an echo.
Q: How often do I need follow-up echocardiograms?
This depends entirely on what the echo shows. A single normal echo in a low-risk individual may not need repeating for many years. Patients with valve disease, cardiomyopathy, aortic aneurysm, or heart failure typically require annual or biannual monitoring. Your cardiologist will advise the appropriate surveillance interval for your condition.
Q: Is echocardiography available in Patna?
Yes. Echocardiography is available at Vikram Heart Care Centre, Dr K K Kantha Memorial Hospital, 21 B/3, Patliputra Colony, Patna.
Book a Consultation
Whether you have been referred for an echo by your doctor or would like a cardiac assessment, Dr Kushaal Vikram and the team at Vikram Heart Care Centre are here to help.
📞 +91 893 583 4142 | +91 886 400 4584
📍 21 B/3, Patliputra Colony, Near Pataliputra Golambar, Opp. UNICEF Building, Patna 800 013
🌐 Book online at kanthahospital.com